Skip to content
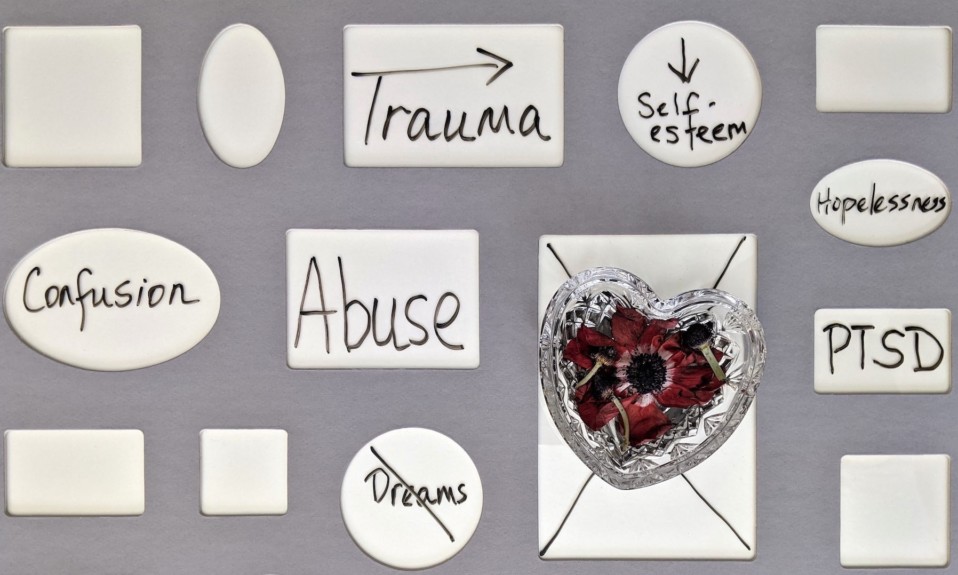
What Is Complex Trauma in Addiction?
The Power of the Recovery Capital Index
Jerry Schwab on Holistic Addiction Treatment
Where Are the Narratives of Healing?
What Is Recovery Capital?
Virtual Reality and the Vision of a Brighter Future
The Profound Significance of Biden’s Marijuana Pardons
Chris Therien: The Puck Stops Here
A Potential Breakthrough in Meth Treatment
How to Sidestep the Trap of News Addiction
What Is Complex Trauma in Addiction?
The Intersection of Prevention and Recovery
What Happens After Out-of-Area Rehab Is Vital
A Double Standard in Addiction Care?
Suicide, Alcohol and Women
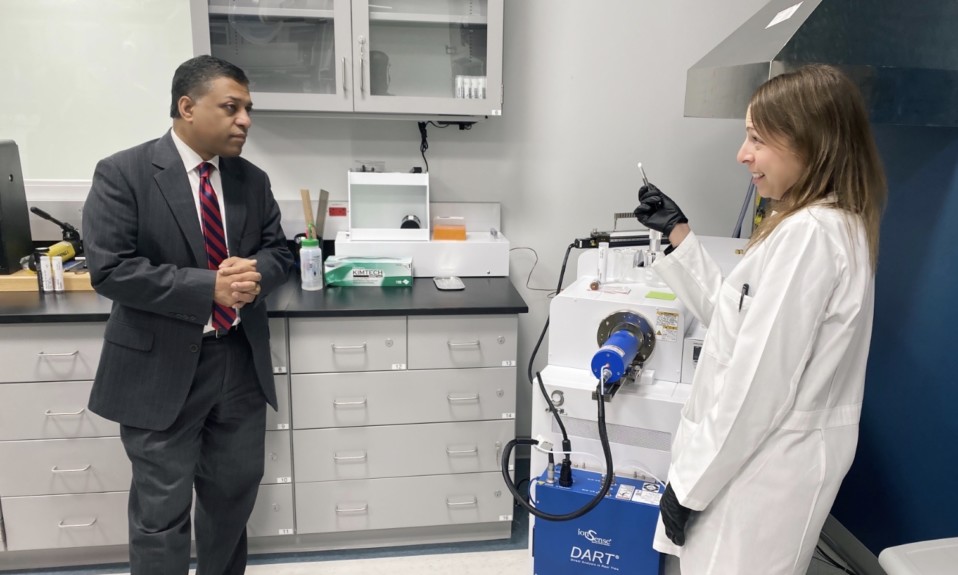
Rahul Gupta, Part II: “This Is No Longer a Partisan Issue”
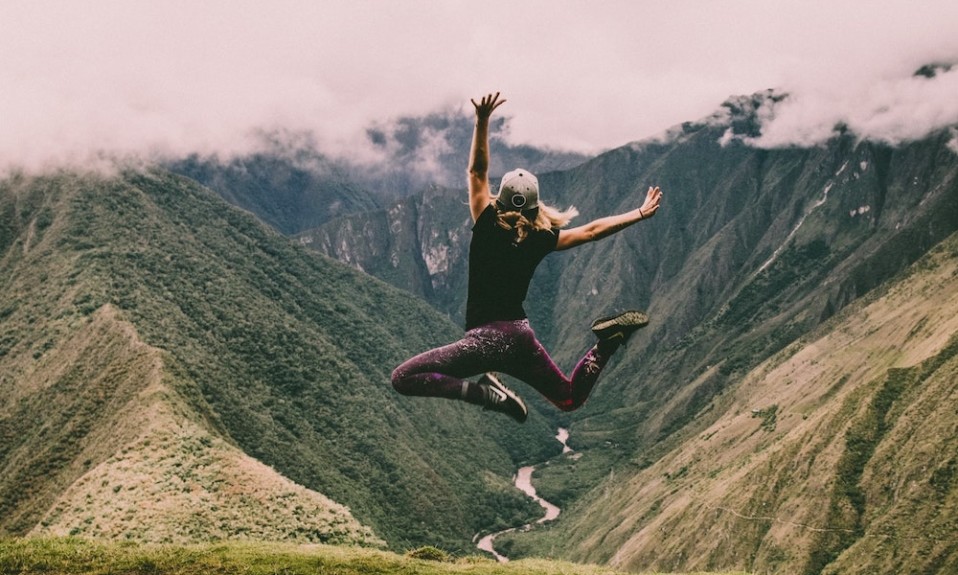
I’m Here to Tell You Recovery Is Possible
What to Do When You Feel Stuck in Addiction
Finding Hope in a Gibson Guitar
Recovery-Friendly Workplaces Increase Productivity
Addiction Treatment Mismatches
Experts: Telehealth Leads to Better Opioid Outcomes
How to Sidestep the Trap of News Addiction